Abstract
Methods
This study used a mixed methods approach to identify perceived enablers and barriers to implementing LSW policies as perceived by school nutrition personnel and other LSW stakeholders. Through a multi-phase Delphi process, a survey with six sections and 63 questions was developed. The survey was pilot tested with school nutrition stakeholders (n=19) and the final survey emailed to all Massachusetts School Food Authorities (n=452). Additionally, the survey was sent to additional stakeholder contacts including the Parent Teachers Association School Nurses Associations, Teachers Association, etc., in Massachusetts. To gain a deeper understanding of the perceptions of barriers and enablers to LSW policy implementation, a sample of survey participants (n=47) was also interviewed by telephone. Descriptive data, including frequencies, were analyzed across survey questions. Qualitative data from the interviews were reviewed for themes.
Results
A total of 948 surveys and 47 interviews were conducted. Most frequently selected peoplerelated enablers included School Foodservice/Nutrition Staff (55%); Administrators (48%); and the School Wellness Committee (40%). Frequently cited process-related enablers included current district/school wellness policy (e.g., what is included; 53%); current district/school wellness policy implementation (e.g., how the policy is implemented; 53%); overall nutrition and physical activity resources (46%); overall school wellness (emotional, mental and social) resources (46%); and coordination of services related to health and wellness (39%). Common survey people-related barriers related included parents/families (52%); classroom teachers (52%); and administrators (32%). Process-related barriers included foods served at class parties or other social events (54%); and personnel time available for wellness-related activity (44%); and funding for school wellness policy (42%).
Conclusions And Applications
The implementation of school wellness policies is shaped by the many enablers and barriers that schools and stakeholders experience. A variety of people (administrators, teachers, and parents) and processes (food served outside the cafeteria, time, funding) represent areas of opportunities to increase the support of and ultimately implementation of LSW policies. Results of this study will help inform the development of resources to support schools throughout Massachusetts.
Full Issue
In 2004, The Child Nutrition and WIC Reauthorization Act established the requirement for a policy addressing Local School Wellness (LSW) which schools were required to implement by 2006 (Child Nutrition and Women, Infants and Children Reauthorization Act of 2004). The Healthy, Hunger-Free Kids Act (HHFKA) of 2010, and the subsequent 2016 final rule from the United States Department of Agriculture (USDA) outlining LSW policy implementation, further reinforced this mandate (HHFKA of 2010; Food and Nutrition Service [FNS], USDA, 2016a). The purpose of the LSW policy is to promote health, well-being, and ability to learn by supporting healthy eating and physical activity for students throughout the school environment. A LSW policy is a written document developed by local educational agencies to promote the competencies set forth by HHFKA.
Much of the early work surrounding LSW policies focused on combating the rising rates of obesity amongst children and adolescents. Indeed, National Health and Nutrition Examination Survey (NHANES) data from 2005-2006, the year before the policy was first required to be implemented, reported the obesity rate for children and adolescents aged 2-19 was 15.4% (Hedley et al., 2004). By 2015-2016 this rate rose to 18.5%, affecting 13.7 million children and adolescents (Hales, Carroll, Fryar, & Ogden, 2017).
LSW policies have been implemented in schools across the country (Labonté, Laverack, & Baum, 2008; School Nutrition Association, 2007) with assessments conducted to determine the degree to which schools have implemented these policies (Buns & Thomas, 2015; Belansky et al., 2009; Francis et al., 2018; Hood, Colabianchi, Terry-McElrath, O’Malley & Johnston, 2013; Kubik, Farbakhsh, & Lytle, 2011; Longley & Sneed, 2009; Mosson et al., 2019; Probart et al., 2008; Profili et al., 2017; School Nutrition Association, 2007). Moag-Stahlber et al. (2008) conducted a national snapshot of LSW policies with findings indicating that only 68% of policies met the guidelines for the mandate. Of the policies reviewed, only 21% provided information in support of implementation. Budd et al. (2012) indicated that 82% of responding schools made staff aware of the requirements for school wellness policies, but only 56% actually trained staff for policy implementation. Common challenges to implementation included lack of time and funding. Lambert et al. (2010) revealed that more than half of the teachers (n=321) surveyed in one state believed they did not have enough time in the classroom to include nutrition-related components. A recent study by Schuler et al. (2018) examined barriers and enablers to implementation of LSW policies in high and low-income schools and found common barriers included parents/families (e.g., lack of support for and involvement in LSW policies at school and home); federal/state regulations (e.g., policy requirements such as a la carte snack items); staff (e.g. lack of participation and commitment to implementation of LSW polices); time (e.g., competing activities and curricular requirements which reduce capacity to implement LSW polices); and funding (e.g., limited funding for the implementation of wellness activities).
While schools have moved toward implementing wellness policies, results of these have been mixed. Longley and Sneed (2009) examined the effects of the mandate on school districts throughout the US and noted that it was reported nutrition information inclusion within overall curriculum increased from 57% (before mandate) to 81% (after), and that offering nutrition education across all grades increased from 52% to 76% after the mandate. However, Belansky et al., (2009) reported minimal impact of the LSW policy in Colorado low-income elementary schools after implementation. Researchers surveyed 45 schools regarding their nutrition and physical activity polices. Although the researchers reported an increase in the time spent in physical activity education, the time allowed for recess decreased, leaving an overall net decrease in physical activity. Yet, other researchers have found additional positive outcomes including changes in offering unhealthy snacks and beverages (e.g., move away from food/beverages high in fat and sugar) (Belansky et al., 2009; Seo, 2009).
Implementation of an LSW policy is multifaceted requiring not only resources (i.e., financial, staff, time, etc.) but additional factors such as knowledge of the process and goals, awareness of the barriers and enablers, and preplanning for evaluation (Mosson et al., 2019). Barriers and enablers are of particular interest as they may provide further information on what is hindering or aiding schools and stakeholders in the implementation of LSW policies.
While previous research has been conducted into barriers and enablers to implementation of LSW policies (Agron, Berends, Ellis, & Gonzalez, 2010; Fernandes, Schwartz, Ickovics, & Basch, 2019; Longley & Sneed, 2009; Schuler et al., 2018; University of Washington Center for Public Health Nutrition, 2009) this research has not been conducted in Massachusetts (MA). In MA and across the nation, school nutrition programs are accountable for providing evidence of an existing LSW policy including an assessment of the implementation of the policy. Indeed, the administrative review process which is part of the certification each school must go through to ensure compliance with the guidelines of the HHFKA includes questions related to the implementation of LSW policies. Anecdotal information from school nutrition personnel within MA indicated an increased burden placed on school nutrition personnel to manage and monitor the LSW policy, including components outside the normal oversight of school nutrition programs. Therefore, the aim of this research is to determine enablers and barriers to implementation of LSW polices in MA schools.
Methods
This mixed methods study utilized an online survey and telephone interviews to explore perceived barriers and enablers to implementing LSW policies. The study is part of a larger needs assessment conducted in collaboration with the Massachusetts Department of Elementary and Secondary Education (DESE), The John C. Stalker Institute of Food and Nutrition (JSI), the MA School Wellness Initiative for Thriving Community Health (SWITCH) Coalition, and the Food and Nutrition Department at Framingham State University. The broader scope of the needs assessment included current wellness-related practices in addition to enablers and barriers to the implementation of school wellness policies. Framingham State University’s Institutional Review Board Committee approved the study.
Survey Development
The Massachusetts School Wellness Needs Assessment (MSWNA) Survey and methods were adapted from The Maryland Wellness Policies & Practices Project (MWPPP), which included a biennial (every two years) quantitative and qualitative survey (Schuler et al., 2018; Maryland Wellness Policies and Practices Project, n.d.). The survey draft was reviewed for face and content validity through a modified Delphi process including two rounds of review and comments. A panel of school nutrition experts (n=22) including members from DESE, JSI, Faculty from FSU and members of the SWITCH Coalition participated in the validation process.
Following the survey development process, the survey was pilot tested with a convenience sample of MA school nutrition stakeholders including school nutrition directors/managers as well as SWITCH Coalition members, and DESE and JSI staff (n=19). The final survey included a consent form and defined how school wellness committees and school wellness policies should be interpreted within the context of the survey. Additional survey sections included
school/district demographics (eight questions), school wellness policy practices (50 questions,data not shown), school wellness policy enablers (two questions), and school wellness policy barriers (two questions). Enablers (factors that promote the implementation of wellness-related activities in schools) and barriers (factors that hinder the implementation of wellness-related activities in schools) were separated into people-related (e.g., administrators, classroom teachers, community partners, federal regulations, parent/families, etc.) and process-related (e.g., a la carte items sold in the cafeteria, coordination of services related to health and wellness, what’s included in current policies, how current policies are implemented, etc.). Participants were asked to select the top three people-related and top five process-related factors, respectively as related to their district/school. The final section thanked participants and asked for consent to be contacted for a follow-up telephone interview.
A link to the survey was emailed to the School Nutrition Director and the School Wellness Chair at all MA School Food Authorities (n=452). Additionally, all SWITCH Coalition Members received letters from DESE asking members to forward the information on to their contacts (e.g., Parent Teachers Association, School Nurses Association, Teachers Association, etc.). The survey was available for 6 weeks, and a reminder email was sent midway through to encourage participation.
Telephone Interviews
The next phase of the needs assessment (March to April 2019) included qualitative data collected from telephone interviews and occurred after the survey closed. An interview guide was developed based on questions asked in the MWPPP (Schuler et al., 2018; Maryland Wellness Policies and Practices Project, n.d.). Questions regarding barriers and enablers were semi-structured with prompts to help uncover perceptions. For example, interviewers asked “What is the biggest overall enabler/barrier to implementing school wellness policies and practices?” This was followed with a probing question “Can you tell me more about” the enabler/barrier mentioned previously and “Can you elaborate with an example”.
A total of 161 survey participants consented to participate in a telephone interview. The participant list was cross referenced so that only one participant from each school district would be called. A total of 117 districts was identified. Using Research Randomizer (randomizer.org), 60 names were selected from the list.
Three graduate assistants (GA) were trained to conduct the interviews, use audio recording equipment, and take field notes. Each GA was assigned 20 contacts. GAs sent an initial email to the potential participant to coordinate a date and time for the interview. An email reminder for the interview date and time was also generated. Interviews were conducted over a two-month period (March-April 2019). All interviews were audio recorded with participant consent. After conducting the interview, GAs sent a “thank you” email which included a copy of the consent form.
Survey And Interview Analysis
Survey data were analyzed using IBM SPSS Statistics (Version 24). Descriptive data included frequencies. Interviews were transcribed by NVivo transcription services, and GAs reviewed each transcript for clarity against their field notes. Transcripts were analyzed using NVivo
(Version 12) with a codebook with themes based on the initial quantitative survey developed. Two research team members reviewed transcripts. To determine interrater reliability, a random sample of three transcripts was selected and reviewed and analyzed for themes by two researchers. Results from each researcher were compared side by side and discrepancies (less than 95% agreement) were discussed until consensus was reached. Once consensus was reached, the codebook was updated to reflect changes.
Results
A total of 948 surveys was collected and 47 interviews were conducted. Four audio recordings were inaudible, leaving a final sample of 43 interviews.
Characteristics Of Schools And Participants’ Roles Within Schools
Less duplicates, approximately 354 schools are represented: public schools n=247, charter schools n=43, private schools n=39, and other (e.g., residential schools) n=25. Participants’ primary role in their schools during the 2018-2019 school year varied with 29% (n=208) selecting School Food/Nutrition Service, 19% (n=138) School Nurse, 18% (n=130) District Level Administrator, and over 8% (n=60) School Level Administrator. Over three-quarters of respondents (77%, n=527) indicated they were a member of their School Wellness Committee. The overall composition of School Wellness Committees varied with 52% including a School Nurse and 51% including a School Food/Nutrition Service member (Table 1).
Table 1. Characteristics of Schools and Participant’s Roles within Schools
| Characteristic | n | % |
| Type of School (N=873) | ||
| Public | 702 | 80 |
| Charter | 61 | 7 |
| Private | 53 | 6 |
| Other | 57 | 7 |
| Grade Level (N=717) | ||
| K-5 | 85 | 12 |
| K-8 | 63 | 9 |
| 6-8 | 54 | 8 |
| 9-12 | 255 | 36 |
| Other | 260 | 36 |
| Primary Role in School (N=717) | ||
| School food/Nutrition service | 208 | 29 |
| School nurse | 138 | 19 |
| District level administrator | 130 | 18 |
| School level administrator | 60 | 8 |
| Phys Ed teacher | 45 | 6 |
| Health teacher | 42 | 6 |
| Teacher | 15 | 2 |
| Parent | 12 | 2 |
| Community partner | 12 | 2 |
| Wellness committee member | 11 | 2 |
| School counselor | 3 | <1 |
| Other (e.g., wellness teacher,
member of district, health and wellness committee chair, etc.) |
41 | 6 |
| School Wellness Committee Member (N=686) | ||
| Yes | 527 | 77 |
| No | 159 | 23 |
| Characteristic | n | % |
| Composition of School Wellness Committee* | ||
| School nurse | 488 | 52 |
| School food/Nutrition service | 482 | 51 |
| School level administrator | 381 | 40 |
| District level administrator | 370 | 39 |
| Phys Ed teacher | 370 | 39 |
| Parent | 326 | 34 |
| Health teacher | 313 | 33 |
| Teacher | 280 | 30 |
| Community partner | 228 | 24 |
| Wellness committee member | 188 | 20 |
| School counselor | 158 | 17 |
| Don’t know | 101 | 11 |
*Participants were able to select multiple responses. Percentage represents percent of total survey respondents (N=948)
Survey Enablers
Of the 948 total survey participants, 429 responded at least once to the questions about LSW policy enablers. The most frequently chosen items were people-related enablers which included School Foodservice/Nutrition Staff (55%); District/School Level Administrators (48%); and the School Wellness Committee (40%) (Table 2). The most frequently chosen enablers related to school wellness processes were current district/school wellness policy (e.g., what is included in the policy; 3%); current district/school wellness policy implementation (e.g., how the policy is implemented; 53%); overall nutrition and physical activity resources (e.g., curriculum and materials; 46%); overall school wellness (emotional, mental and social) resources (e.g., curriculum and materials; 46%); and coordination of services related to health and wellness (39%).
Survey Barriers
Three hundred forty-five respondents identified at least one barrier. The most frequently selected barriers related to the category of people included parents/families (52%); classroom teachers
(52%); administrators (32%); and students (32%) (Table 2). Barriers related to the category of processes included foods served at class parties or other social events (54%); personnel time available for wellness-related activity (44%); funding for school wellness policy (42%); foods sold by other school groups (38%); and time to plan and coordinate wellness-related activities (37%).
Table 2. Top Survey Enablers and Barriers Related to People, Organizations, Policies, and Programs.
| Enablers (N=429) | Barriers (N=345) | |||
| Top
n (%) |
Top 3
n (%) |
Top
n (%) |
Top 3
n (%) |
|
| Administrators (district/school level) | 85 (20) | 207 (48) | 59 (17) | 112 (32) |
| Classroom teachers | 17 (4) | 84 (20) | 61 (18) | 178 (52) |
| Community Partners | 5 (1) | 40 (9) | 5 (1) | 21 (6) |
| Federal Regulations | 37 (9) | 73 (17) | 38 (11) | 84 (24) |
| Local/National health promotion
organizations |
3 (1) | 18 (4) | 2 (.5) | 8 (2) |
| Other School Staff | 11 (3) | 72 (17) | 17 (5) | 94 (27) |
| Parents/Families | 8 (2) | 38 (9) | 71 (21) | 179 (52) |
| PE teachers | 39 (9) | 107 (25) | 2 (.5) | 6 (2) |
| School Counselors | 3 (1) | 21 (5) | 1 (.5) | 1 (.5) |
| School foodservice/Nutrition staff | 84 (20) | 237 (55) | 8 (2) | 29 (8) |
| School Wellness committee | 70 (16) | 170 (40) | 5 (1) | 17 (5) |
| School Wellness committee chair | 35 (8) | 70 (16) | 3 (.5) | 6 (2) |
| State Regulations | 27 (6) | 90 (21) | 23 (6) | 84 (24) |
| Students | 3 (1) | 20 (5) | 38 (11) | 111 (32) |
Interview Enablers
The top three themes for enablers were people (n=42), school wellness culture (n=19), and implementation of school wellness policy (e.g., how policy is implemented; n=12). Within the theme of people, administrators were mentioned frequently as important factors with 35 references (ref=35). “If you don’t have a good strong administrative support group… then you can’t justify… asking people to initiate wellness
programs…You need those people [administrators] to back you up and to…offer funding and to say ‘yes, these are important’.” Having a wellness committee was also cited
(ref=35) as an important enabler. “…[We have] members that are dedicated to the wellness team…they not only participate in the district wellness team but they have wellness teams within each of their own schools so that they can really implement the wellness activities that we desire but also help to make sure that people are following the wellness policy.” Parents and families were also mentioned (ref=24) as important factors in implement LSW policies. “…we can expose students to a lot of different ideas and foods and healthy concepts. But parents really taking the next step is super important.”
Interview Barriers
The top three themes related to barriers included implementation of wellness policy (e.g., how the policy is monitored, n=42); people (e.g., who acts as a barrier to implementation of LSW policies and who monitors/implements policy, n=25); and food availability (e.g., availability of food at school in classrooms or at events/sold through fundraisers, and at home that does not meetg federal and state guidelines, n=19). Participants indicated implementing or enforcing the food-related rules was a challenge. We think we draft a pretty good policy. But who is the person that actually says to that high school teacher, “You can’t be serving those doughnuts”. Other issues included being able to translate the policy into practice. …if the parent isn’t going to follow the rules…it’s not like they’re breaking a big law. They can feed their kids what they want…So a wellness policy is only as good as selling it. And then people buying into it. Some respondents mentioned the idea of people working in vacuums or not being aware of the policies and then violating the policy because no one is overseeing. [When there’s a basketball game] they’re selling candy and that’s all a violation of the Wellness Policy… the nurse leader helped make the policy, [but the question among the nurses has been] who is going to police it?
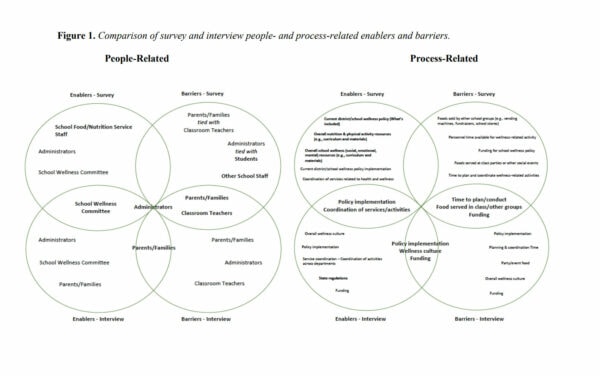
Comparison Of Survey And Interview Enablers And Barriers
There were several commonalities across survey and interview top responses. Among people-related responses, all survey and interview participants indicated administrators were perceived as both an enabler and barrier. In addition, the school wellness committee was mentioned as a top enabler by both groups while parents/families and classroom teachers were mentioned as barriers (Figure 1).
Survey and interview participants also identified similar key process-related enablers and barriers. Policy implementation and coordination of services/activities were selected as enablers by both groups. Additionally, selections related to time (time to plan and coordinate or personnel time for activities); food (foods served by other school groups and at classroom parties or other social events); and funding for wellness policies were common barrier themes across both groups (see Figure 1).
Discussion
People-related barriers included parents/families, teachers, administrators, and students, while key process-related barriers included foods served outside of the cafeteria, monetary funds, and resources. These findings support previous research (Longley & Sneed, 2009; Schuler et al., 2018). In this current study, administrators are considered an enabler and a barrier by both survey and interview participants, implying that district/school administrators set the tone and have the power to create, direct, and instill a positive wellness culture. This finding is similar to Schuler et al. (2018) in which researchers indicated that school staff served as both a barrier and enabler to policy implementation. Profili et al. (2017) examined wellness-related best practices and found that including key personnel (e.g., school administrators) was one practice resulting in a higher degree of school wellness policy implementation. Similarly, to administrators, in the current study teachers are identified as barriers to the implementation of LSW policies, as lack of support from educators often revolved around food. A study by Fernandes et al. (2019) indicated that teachers may be more attuned to food insecurity and hunger and cultural norms of students and families. For example, teachers may provide students with snacks in classrooms because students may not have eaten since the previous day. Likewise providing food-based classroom celebrations may be deemed as a cultural component of the school environment or may be tied to an inherent reward based food culture which is seen as difficult to overcome. Teachers may need further assistance in addressing these issues before they would buy-in to restricting any food in the classroom.
Parents may also be important stakeholders in helping to foster a culture of school wellness, and yet, they are perceived as a barrier in this study. Hildebrand et al. (2019) examined the connection between parents’ perceptions of childhood obesity and their support of school wellness policy, and found that while parents may perceive obesity as a statewide issue, they did not perceive a problem with their own school or area. This sense of “not in my community” may help explain the lack of buy-in or support schools may feel from parents regarding LSW policies.
Conclusions And Applications
All school districts participating in the National School Lunch Program and/or the School Breakfast Program are required to have a LSW policy (FNS, USDA, 2016a). The MSWNA provides a template for understanding the factors that hinder and aid the implementation of LSW policies.
School wellness policies need the support of district/school level administrators. Based on the findings of this study, administrators may be key stakeholders in driving LSW. Although the current research does not further elucidate the factors influencing administrators and staff specifically, additional barriers indicated by respondents included funding and time. These factors are supported by the work of Cox et al., (2011) who indicated limited resources such as school budget, time to plan and complete training and activities, and prioritization of alternate needs influence administration support of school wellness policies. It may be that a targeted approach to administrators, outlining the benefits and the return on investment (in terms of positive impacts of school wellness policies) may be keys to developing support and buy-in.
School wellness policies need engaged teachers to help implement policies. Classroom, health, and physical education teachers are key players in the overall wellness environment. Students spend much of their school day in classrooms and their teachers are responsible for creating an environment conducive to learning which may be enhanced by wellness factors. Research shows that classroom environments and academic achievement are directly reflective of social and emotional wellbeing (Darling-Hammond, Flook, Cook-Harvey, Barron, & Osher, 2019) which are key components of wellness policies. This reinforces the necessity of engaging and supporting teachers in implementing practices which reinforce LSW policies. However, teachers are already overburdened and under pressure to meet the academic criteria set out for them, and schools do not always have the extra resources (time, money, and people) that can be allocated to teachers to help implement wellness-related activities. Indeed, it may be that teachers support and even want to incorporate wellness-related activities; however, they lack the tools and resources to do so. Research by Lambert et al. (2010) indicates that while teachers understood the importance of LSW policies they did not have time to incorporate nutrition competencies into the curriculum, and they did not see themselves as stakeholders in policy changes. In addition to providing resources such as time and money, including teachers in the planning process may help move these important stakeholders from opponents to proponents of school wellness. In order to engage teachers in the implementation of LSW policies, schools will need to meet teachers where they are – in the classroom with free, simple, and readily available resources that can be easily integrated into existing curricula.
School wellness policies need an active school wellness committee. Wellness policies need a broad group of advocates (parents, students, teachers, etc.) and having a defined, dedicated, and active school wellness committee that reflects these diverse roles may also make it easier for schools to engage stakeholders who can help implement policies. Likewise having wellness committee members who role model healthy behaviors in the school can provide foundational learning experiences for students. For example, wellness committee members who eat school lunch with students in the cafeteria, attend physical activity events, and outreach to parents/guardians are messaging healthy behaviors. Continued support for districts/schools who currently have a wellness committee fully or partially in place is important, but equally important is leveraging the achievements of successful districts/schools to help others.
School wellness policies need to support school foodservice/nutrition programs. Because the administrative review process requires school nutrition programs to document the progress of LSW policies, it is not surprising that school foodservice/nutrition staff would be thought of as enablers in the process. In order for school foodservice/nutrition staff to continue in their roles of promotors and advocates of school wellness, this important group needs to be supported in terms of key process-related enablers (e.g., time to participate in wellness-related activities and money to implement wellness-related policies). For example, LSW policies provide guidance on the marketing of a la carte foods (foods sold in the cafeteria, school stores/snack bars, and vending machines) and prohibit the sale of foods that do not meet Smart Snack Standards (e.g., snack that is 200 calories or less, 200 mg or less of sodium, 35% calories or less of total fat, etc.) (FNS, USDA 2019). Yet, food and nutrition departments rely on a la carte sales to supplement revenue and reimbursement monies to sustain their operations. This puts school food and nutrition programs in a precarious position of balancing support of initiatives and revenue to maintain operations. While LSW policies include many important areas that directly impact the overall well-being of students, nutrition is a foundational component tied directly to the initial intended goals and objectives (i.e., reduce the rate of childhood obesity) of the mandate. Therefore, continued attention to barriers that impact school nutrition programs must remain a priority. Likewise, support for foodservice/nutrition staff must continue to be provided to help achieve LSW policy aims.
An appropriate process to assist with implementation of school wellness policies was identified in this study. Although people are very important in making a policy happen, processes must be in place to guide actions. Elements of the policy, how the policy is implemented, and resources allocated to implementation (e.g., funding) were all identified as important enablers, by both survey and interview participants. These factors may predict the success or degree of success a school may have in implementing and executing their policy and warrant further research. The dedication of resources including time to plan and implement and funding to support initiatives may be crucial in providing the support needed to move schools toward the goals of their individual LSW policies. Additionally, the continued development of training resources that feature the best practices of top enablers of people and processes across the wellness spectrum should be a priority to help keep a positive momentum going forward. Distinct barriers to the implementation of school wellness policies were reported, including time to plan or conduct activities, the challenge of foods served/sold in classrooms or sold by other groups that do not meet state and federal guidelines, and lack of funding for wellness policies. These challenges may continue without internal (administration, teacher, parent, and student) and external (funding, and state and federal resources) support. While continued support of schools who currently have a wellness committee fully or partially in place is important, equally important is leveraging the successes of these schools to help others.
School wellness is everyone’s responsibility. The implementation of LSW policies is shaped by the many enablers and barriers that schools experience. For example, while schools need the support of administrators, teachers, and parents, schools also need free, convenient, and easy to use resources and tools that will reduce the current burdens of developing and implementing wellness policies. Therefore, shifting the wellness culture within schools may take time and may be related to the positive actions of people and processes. In many instances, people and processes act as both enablers and barriers, indicating the importance of framing wellness as a comprehensive multifaceted effort in order to create a culture where school wellness really is everyone’s responsibility. Additionally, the core objective of LSW policies is to address the rising rates of obesity within the context of traditional physical activity and nutrition (e.g., the cafeteria) programs. However, foundational tenets of physical activity and nutrition can also be integrated into activities and areas across the school environment. For example, providing cross-curricular instruction for nutrition and physical activity education in science, math, etc., is just one way to integrate wellness-related components (FNS USDA, 2016a). This is a monumental task and one that requires the input and dedication of many people and processes within the school setting further reinforcing that school wellness is everyone’s responsibility.
Limitations of this study include potential response bias from both the survey and interview participants. Furthermore, participants in the interview were chosen from a pool of self-selected respondents, from one state (MA) indicating possible selection bias, although, in an effort to minimize the impact of this potential bias, interview participants were randomly selected from the pool. Additionally, surveys were sent to 452 school districts (School Foodservice Directors and School Wellness Chairs), and were further distributed by SWITCH Coalition members. This approach makes it difficult to calculate a response rate and may miss including important groups. Despite these limitations, the findings of this study were strengthened by the mixed methods approach using both quantitative and qualitative research. This method helps give voice to numbers and balances the strengths and weaknesses of each method (Tariq & Woodman, 2013). In addition, through a modified Delphi process researchers adapted a previously developed and implemented study protocol and assessment tool to reflect the general activities and environment of MA schools.
Future research should look to uncover the reasons why both people (administrators, teachers, students, etc.) and processes (how policies are implemented, food served outside the cafeteria, resources, etc.) act as barriers. Likewise, it will be important to understand and analyze by characteristics (e.g. grade level) the best practices of schools that report being successful in engaging people and utilizing processes to implement LSW policy. The results of the Massachusetts School Wellness Needs Assessment will be used to guide the development of resources (e.g., wellness coaching model and website) to support schools throughout the Commonwealth of MA.
Acknowledgments
This work was funded through the United States Department of Agriculture’s National School Lunch Program, as administered by the Massachusetts Department of Elementary and Secondary Education, Office for Food and Nutrition Programs and the Food and Nutrition Department at Framingham State University. The authors would like to thank the SWITCH Coalition members and the staff of The John C. Stalker Institute of Food and Nutrition and the Massachusetts Department of Elementary and Secondary Education, Office for Food and Nutrition Programs who participated in the Delphi process. Additionally, we would like to acknowledge the hard work and dedication of the Framingham State University, Department of Food and Nutrition Graduate Assistants for their contributions to this work.
References
Agron, P., Berends, V., Ellis, K., & Gonzalez, M. (2010). School wellness policies: Perceptions,
barriers, and needs among school leaders and wellness advocates. Journal of School Health
80(11), 527-535.
Belansky, E. S., Cutforth, N., Delong, E., Ross, C., Scarbro, S., Gilbert, L., . . . Marshall J. A.
(2009). Early impact of the federally mandated local wellness policy on physical activity in
rural, low-income elementary schools in Colorado. Journal of Public Health Policy, 30(S1),
S141-S160. https://doi.org/10.1057/jphp.2008.50
Budd, E. L., Schwarz, C., Yount, B. W., & Haire-Joshu, D. (2012). Factors influencing the
implementation of school wellness policies in the United States, 2009. Preventing Chronic
Disease, 9, E118. http://dx.doi.org/10.5888/pcd9.110296
Buns, M. T., & Thomas, K. T. (2015). Impact of physical educators on local school wellness
policies. The Physical Educator, 72(2), 294. Retrieved
from https://search.proquest.com/docview/1700479018
Child Nutrition and Women, Infants, and Children Reauthorization Act of 2004. Pub L No 108-
265, June 30, 2004, (118 Sta 729).
Cox, L., Berends, V., Sallis, J. F., St John, J. M., McNeil, B., Gonzalez, M., & Agron, P. (2011).
Engaging school governance leaders to influence physical activity policies. Journal of
Physical Activity & Health, 8 Suppl 1(s1), S40-S48. https://doi.org/10.1123/jpah.8.s1.s40
Darling-Hammond, L., Flook, L., Cook-Harvey, C., Barron, B., & Osher, D. (2019).
Implications for educational practice of the science of learning and development. Applied
Developmental Science. https://doi.org/10.1080/10888691.2018.1537791
Fernandes, C. F., Schwartz, M. B., Ickovics, J. R., & Basch, C. E. (2019). Educator perspectives:
Selected barriers to implementation of school-level nutrition policies. Journal of Nutrition
Education and Behavior, 51(7), 843-849. https://doi.org/10.1016/j.jneb.2018.12.011
Food and Nutrition Service [FNS], USDA. (2016a), Local School Wellness Policy
Implementation Under the Healthy, Hunger-Free Kids Act of 2010. Final rule. Federal
Register. 81(146), 50151-50170. Retrieved from http://www.fns.usda.gov/schoolmeals/fr072916c
Food and Nutrition Service [FNS], USDA. (2019). A Guide to Smart Snacks in School 2019-
2020. FNS-623. Retrieved from https://fns-prod.azureedge.net/sites/default/files/resourcefiles/USDASmartSnacks_508_62019.pdf.
Francis, E., Hivner, E., Hoke, A., Ricci, T., Watach, A., & Kraschnewski, J. (2018). Quality of
local school wellness policies for physical activity and resultant implementation in
Pennsylvania schools. Journal of Public Health (Oxford, England), 40(3), 591-597.
https://doi.org/10.1093/pubmed/fdx130
Hales, C. M., Carroll, M. D., Fryar, C. D., & Ogden, C. L. (2017). Prevalence of obesity among
adults and youth: United states, 2015-2016. NCHS Data Brief, (288), 1. Retrieved
from https://www.cdc.gov/nchs/data/databriefs/db288.pdf
Healthy, Hunger-Free Kids Act of 2010, Pub. L. No. 111-296 (2010).
Hedley, A. A., Ogden, C. L., Johnson, C. L., Carroll, M. D., Curtin, L. R., & Flegal, K. M.
(2004). Prevalence of overweight and obesity among US children, adolescents, and adults,
1999-2002. JAMA, 291(23), 2847-2850.
Hildebrand, D. A., Betts, N. M., & Gates, G. E. (2019). Parents’ perceptions of childhood
obesity and support of the school wellness policy. Journal of Nutrition Education and
Behavior, 51(4), 498-504. https://doi.org/10.1016/j.jneb.2018.12.009
Hood, N. E., PhD, Colabianchi, N., PhD, Terry-McElrath, Y. M., MSA, O’Malley, P. M., PhD,
& Johnston, L. D., PhD. (2013). School wellness policies and foods and beverages available
in schools. American Journal of Preventive Medicine, 45(2), 143-149.
https://doi.org/10.1016/j.amepre.2013.03.015
Kubik, M. Y., Ph.D, Farbakhsh, K., M.S, & Lytle, L. A., Ph.D. (2011). Two years later:
Wellness councils and healthier vending in a cohort of middle and high schools. Journal of
Adolescent Health, 49(5), 550-552. https://doi.org/10.1016/j.jadohealth.2011.03.011
Lambert, L. G., Monroe, A., & Wolff, L. (2010). Mississippi elementary school teachers’
perspectives on providing nutrition competencies under the framework of their school
wellness policy. Journal of Nutrition Education and Behavior, 42(4), 271-276.e4.
https://doi.org/10.1016/j.jneb.2009.08.007
Longley, C. H., & Sneed, J. (2009). Effects of federal legislation on wellness policy formation in
school districts in the United States. Journal of the American Dietetic Association, 109(1),
95-101. https://doi.org/10.1016/j.jada.2008.10.011
Maryland Wellness Policies and Practices Project. (n.d.). Retrieved from
http://www.marylandschoolwellness.org/Projects/Maryland-Wellness-Policies-andPractices-Project/
Moag-Stahlberg, A., Howley, N., & Luscri, L. (2008). A national snapshot of local school
wellness policies. Journal of School Health, 78, 562-568.
Mosson, R., Augustsson, H., Back, A., Ahstrom, M., Schwarz, U., Richter, A., . . . Hasson, H.
(2019). Building implementation capacity (BIC): A longitudinal mixed methods evaluation
of a team intervention. BMC Health Services Research, 19(1), 287. Retrieved
from h http://kipublications.ki.se/Default.aspx?queryparsed=id:140837280
Profili, E., Rubio, D. S., Lane, H. G., Jaspers, L. H., Lopes, M. S., Black, M. M., & Hager, E. R.
(2017). School wellness team best practices to promote wellness policy
implementation. Preventive Medicine, 101, 34-37.
https://doi.org/10.1016/j.ypmed.2017.05.016
Ronald Labonté, Glenn Laverack, & Fran Baum. (2008). Health promotion in action. GB:
Palgrave Macmillan. Retrieved
from https://ebookcentral.proquest.com/lib/[SITE_ID]/detail.action?docID=455184
School Nutrition Association. (2007). From cupcakes to carrots: Local wellness policies one
year later. Retrieved from
https://schoolnutrition.org/uploadedFiles/5_News_and_Publications/4_The_Journal_of_Chil
d_Nutrition_and_Management/Fall_2010/From_Cupcakes_to_Carrots.pdf
Schuler, B. R., Saksvig, B. I., Nduka, J., Beckerman, S., Jaspers, L., Black, M. M., & Hager, E.
R. (2018). Barriers and enablers to the implementation of school wellness policies: An
economic perspective. Health Promotion Practice, 19(6), 873-883.
https://doi.org/10.1177/1524839917752109
Seo, D. (2009). Comparison of school food policies and food preparation practices before and
after the local wellness policy among Indiana high schools. American Journal of Health
Education, 40(3), 165-173. https://doi.org/10.1080/19325037.2009.10599091
Tariq, S., & Woodman, J. (2013). Using mixed methods in health research. JRSM short reports,
Retrieved from https://doi.org/10.1177/2042533313479197
Probart, C., McDonnell E., Weirich E. J., Schilling L., & Fekete V. Statewide assessment of
local wellness policy in Pennsylvania public school districts. (2008). Journal of the
American Dietetic Association 108, 1497-1502.
University of Washington Center for Public Health Nutrition. (2009).
Barriers to school wellness policy implementation. Retrieved from https://nutr.uw.edu/wpcontent/uploads/2009/11/barriers.pdf
Biography
The Authors are all at Framingham State University in Framingham, Massachusetts. Catherine A. Wickham, PhD, RDN, CDN is Assistant Professor in the Food and Nutrition Department at Framingham State University in Framingham, Massachusetts and Faculty Liaison to The John C. Stalker Institute of Food and Nutrition. Michael Crosier, PhD, RD is an Associate Professor in the Food and Nutrition Department and Megan Lehnerd, PhD, MS, is an Assistant Professor in the Food and Nutrition Department, both at Framingham State University. Karen McGrail, MEd, RDN, LDN, is Director of The John C. Stalker Institute of Food and Nutrition. Denise Courtney, MS, RD, SNS, is a Nutrition Education and School Wellness Training Coordinator in the Office for Food and Nutrition Programs of the Massachusetts Department of Elementary and Secondary Education. Nicole Good is a School Wellness Specialist in the Office for Food and Nutrition Programs of the Massachusetts Department of Elementary and Secondary Education.
Purpose / Objectives
The aim of this study is to determine the enablers and barriers to implementation of local school wellness (LSW) policies in Massachusetts schools. Findings will help inform the development of resources to support school nutrition directors and other important stakeholders who have the potential to influence implementation of these policies.