Abstract
Methods
Researchers created training materials based on IDDSI resources. A convenience sample (N=59) of university nutrition students as a proxy for child nutrition line-level staff were trained on diet standards and procedures. Food and beverage products were prepared and assessed. A feedback questionnaire and taste tests comparing food items prepared by students with commercially prepared products were conducted.
Results
Participants effectively prepared and assessed texture-modified items. A range of successfully completed assessment forms was observed (35-94%), indicating the need for repeated instruction and practice. Positive feedback was received regarding the procedures. Student-prepared food items were preferred over their commercial counterparts.
APPLICATION TO CHILD NUTRITION PROFESSIONALS
Use of IDDSI-based materials by child nutrition personnel in school settings is viable. Use of developed guidance may support increased food acceptance and nutritional intake among students requiring texture-modified diets.
Full Issue
Dysphagia is the term used to describe various degrees of swallowing difficulties with food and liquids (National Institute on Deafness and Other Communication Disorders, 2010). There is an estimated 2.8 million school children in the United States with a range of disabilities (United States Department of Agriculture Food and Nutrition Service [USDA FNS], 2017); an estimated 25-80% of these children with developmental disorders require a texture-modified diet for dysphagia (USDA FNS, 2017). Federal law requires public schools to provide accommodations, including the provision of a texture-modified diet, to ensure children’s needs are met (Arvedson, 2008; USDA FNS, 2017).
Consequences of dysphagia include dehydration and poor nutritional intake as eating is difficult, frustrating, and tiring, often resulting in reduced consumption (Dodrill & Gosa, 2015). Children who do not receive adequate nutrition may experience inadequate growth and delays in mental, physical, and social development (Failure to Thrive, 2017). These children may perform poorly on academic measures (Holben, 2010). In addition, dysphagia increases the risk for choking and aspiration if food or liquid enters the lungs, possibly resulting in pneumonia (Matsuo & Palmer, 2008). Such consequences illustrate the need for properly prepared school menu items that are acceptable to children participating in child nutrition programs.
To receive school-based dysphagia services, the student, family representative(s), and school staff must engage in a collaborative evaluation process. Under the 2004 reauthorization of Individuals with Disabilities Education Act (IDEA), schools are required to provide accommodations for children with disabilities such as dysphagia (USDA FNS, 2017). Such accommodations include texture-modified meals, yet accessible public information regarding how child nutrition programs are providing texture-modified foods and student consumption has been limited. The provision of school-based dysphagia services is further complicated by constraints of availability and retention of trained staff (Edgar & Rosa-Lugo, 2007; Homer 2008; Homer & Carbajal 2015; Hoffman, Srinivasan, Levan, & Scarmo, 2018).
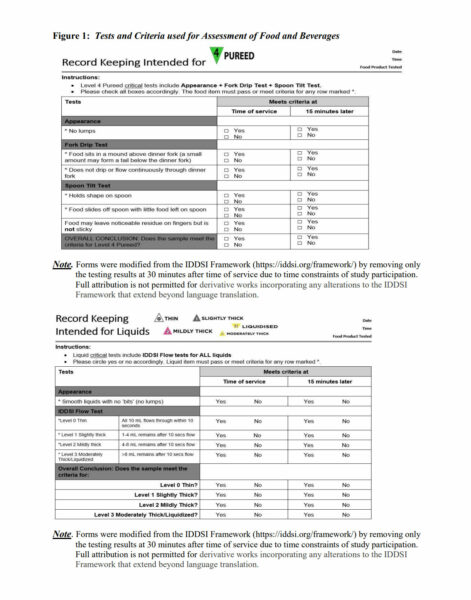
Guidelines for dysphagia have recently been updated by an international group of healthcare professionals to better the care and wellbeing of individuals with dysphagia. In 2013, the International Dysphagia Diet Standardisation Initiative (IDDSI) classification system was formed to provide standardized terminology and criteria to describe texture-modified foods and thickened liquids for individuals with dysphagia. The IDDSI identified eight levels of texture-modified foods and thickened liquids and provided detailed descriptions of characteristics and methodologies for testing whether the food or liquid met the IDDSI target level (IDDSI, 2016). For example, the Level 4 pureed examined in this study requires the food to have no lumps, to show only slow movement under gravity but not be able to be poured, cannot be sucked through a straw, and be able to hold its shape on a plate. This level of thickness is needed for those who have reduced tongue control. Testing methods recommended by the IDDSI include the Appearance Test, Fork Test, Flow Test, and Spoon Tilt Test. The Level 2 Mildly Thick items must flow off a spoon, be sippable, and require mild effort to drink through a standard straw. Testing this level requires a Flow Test through a syringe.
The Academy of Nutrition and Dietetics and the School Nutrition Association support increased resources and training to better assist schools with development and implementation of strong nutrition services addressing students with dysphagia (Hayes, Contento, & Weekly, 2018). Thus, there is a need to provide education and training for child nutrition personnel on production of texture-modified food and beverage menu items, and on evaluation of texture level criteria of the IDDSI classification system.
According to the American Speech-Language-Hearing Association (ASHA), social factors such as pleasure (acceptance) and fear related to food and food textures should be considered when choosing treatment plans, including a pureed diet, for dysphagia patients (ASHA, 2010). In their review of the literature, Guerrero, Olsen, and Wistoft (2018) found the focus of school food service studies centered around increasing fruit and vegetable consumption, with a lack of studies relating to the influence of food acceptance on physical and psychological well-being. Limited data is available on pureed food acceptance by children with most published research on adults and elderly patients. Studies pertaining to elderly dysphagia have found that when pureed meals were modified to increase acceptance, caloric intake and patient body weight increased as a result (Germaine, Dufresene, & Gray-Donald, 2006; Amunrud, Mitchell, & Sun, 1999). Among children, Wadhera and Phillips (2014) and Werthmann et al. (2015) found that visual cues were critical to food acceptance. While DeSantos et al. (2010) investigated the importance of multiple sensory characteristics in children and reported that appearance, texture, and taste were important to food acceptance of pureed salmon, a gap in the dysphagia- related literature regarding provision and acceptance of texture-modified foods in child nutrition programs still exists. Therefore, the purpose of this study was to evaluate publicly available materials developed by the IDDSI for feasibility of use by child nutrition programs and the acceptance of developed standardized pureed recipes.
METHODOLOGY
This study included two phases: Development and Training/Testing. A convenience sample of university students enrolled in four food and nutrition related classes one university school was solicited for volunteer participation in the Training /Testing phase of the study. University nutrition students served as a proxy for child nutrition line-level personnel. In addition to the availability of the student sample, it was believed students would have limited experiences with producing texture-modified foods and would serve as a reasonable proxy for child nutrition personnel. The researchers recruited participants from a pool of 92 students, including the new graduate student class of dietetic interns who were recent graduates of a Didactic Program in Dietetics. Students excluded were those with identified food allergies or intolerances. A total of 59 students volunteered to participate. Study activities took place in the University Food Laboratory and adjacent dining room. The study was conducted in the summer and fall of 2018, after approval of all materials and procedures by the Institutional Review Board.
Phase I: Development of Education Materials and Recipes
Education Materials
Education materials were modified based on publicly available guidelines and resources presented by the IDDSI (2016). To ensure the information was communicated clearly to all participants, the education materials were evaluated for readability using the SMOG formula
(McLaughlin, 1969) which assigns a grade reading level to written materials. The target reading level was 6th – 8th grade. Nutrition faculty also reviewed the materials for content validity with revisions made per their suggestions. In addition, the researchers developed a short, 15-item feedback questionnaire for students to assess their perceptions of the training and feasibility of product testing procedures. The feedback form also captured participants’ characteristics.
Recipes
Researchers developed four standardized pureed recipes typical to school menus that met the criteria for a Level 4 Pureed Diet. This level was selected because it is the first level in the continuum that cannot be drunk from a cup and requires additional skills in food preparation and evaluation not typical to all child nutrition programs, such as conducting a fork drip test. A commercial thickener (Thick-It Ⓡ Original Thickener) was used to alter the texture and consistency of the items. The Level 2 Mildly Thick liquids was chosen for this research project as it represents the mid-range of the thickness scale, is sippable, and flows off a spoon. This level requires testing not typically utilized in child nutrition programs, such as the Flow Test utilizing a syringe. Testing of the food and beverage products followed the methodologies outlined in the IDDSI Framework (IDDSI, 2016). Pureed recipes were developed for menu items reflective of school meal components with inclusion of one fruit, vegetable, grain, meat, and milk product: peaches, carrots, macaroni and cheese, and spaghetti with meatballs.
Phase II: Training and Testing
Study participants first received a 25-30 minute presentation developed by the researchers on the diet standards of the IDDSI, followed by instruction on preparation methods including the addition of a commercial thickener, procedures for assessment of products, and consistency testing equipment. Next, participants prepared and assessed the new recipes using the Appearance Test, Fork Test, Flow Test, and Spoon Tilt Test. Participants also evaluated the frozen, reheated recipes previously prepared by the researchers using the same tests, and compared these to similar commercial products.
Criteria used for these tests were developed by IDDSI in 2016 and are shown in Figure 1 (Level 4 Pureed Foods and Level 2 Mildly Thick Liquids). These forms were modified slightly to correspond with the procedures of this study. Specifically, the IDDSI forms state items should be tested at the time of service, 15 minutes later, and 30 minutes after the time of service. The latter testing time of 30 minutes was removed from the form so as not confuse the participants. Following testing of items, participants completed the feedback questionnaire regarding their perceptions of the experience.
After the assessments of the menu items from developed recipes were completed and feedback regarding their experiences was obtained, participants completed a taste test of the pureed food products produced by the researchers and a similar, commercially purchased product. The researcher-prepared items were used in the taste tests in order to have consistency in flavor and texture for the comparison. For this study, commercial baby foods packaged in sealed, shelf-stable jars were used. For example, the previously prepared and frozen pureed carrots were compared to pureed carrots purchased commercially (baby food). A review of the nutrient fact panels found that the sodium levels were similar for the frozen carrots and the baby food, however, when preparing the frozen carrots, salt was added. The researchers left the taste testing site so as not to influence the results and to maintain participant anonymity. Samples were labeled “A” or “B” to conceal their method of preparation. Participants completed a nine-point hedonic scale sensory evaluation with ratings from “Like Extremely” to “Dislike Extremely” for each food product after tasting the items (carrots, peaches, spaghetti with meatballs, macaroni and cheese). Sensory components included taste, smell, appearance, and texture (Vaclavik & Christian, 2014). Participants were instructed to consume a cracker and sip water prior to repeating the procedure for subsequent samples. The item evaluation concluded with a paired preference test that asked participants to briefly explain the reason for choosing the preferred sample. Participants placed completed forms in a folder to maintain anonymity. The researchers viewed the forms upon completion of the data collection.
Data Analysis
Descriptive statistics were used to analyze data collected from menu item evaluation forms and participant questionnaires. Mean scores were calculated for all sensory characteristics. Analyses was conducted using the IBM Statistical Package for the Social Sciences (SPSS) software, Version 22 (IBM Corp, 2013).
RESULTS AND DISCUSSION
Profile of Respondents
The majority of the 59 participants was female (85%), a senior-level student (46%), and between the ages of 19-23 years (54%), although the age range was 19-53 years. Most (81%) stated they had not received previous training in producing foods modified in texture or consistency. This finding is valuable as the perspective of the untrained student served as a proxy for a newly hired food service employee. Participants that did report prior training indicated either a family member required a modified diet, they had worked in a healthcare facility, or had received training in academic classes or through the dietetic internship.
Level 4 Pureed Foods
As seen in Table 1, participants were most successful at producing pureed carrots and peaches using the developed recipes, as these items met the Level 4 criteria in 79-83% or more of the assessments. The researcher-produced, thawed carrots and peaches met the Level 4 criteria in 83-100% of the assessments. Most participant-produced meatballs, and macaroni and cheese items did not achieve Level 4 Pureed criteria (44-46% and 29-36%, respectively), possibility related to the need for additional time necessary to fully puree these items. However, the thawed, researcher-produced meatballs and the macaroni and cheese showed increased proportions of samples meeting Level 4 Pureed standards by comparison (62-74% and 33-63%, respectively). The percent of correctly completed food item assessment forms 35-94% noted.
These forms required participants to indicate whether or not each food item met the Appearance, Fork Drip, and Spoon Tilt tests. The most common reasons for incorrect completion of the forms were missing responses and the inability of the participants to identify whether the food item met the criteria for Level 4 pureed foods after marking the results of each criteria test. This finding is not surprising given the limited training (the 25-30 minute presentation by researchers) and limited experiences with modified diets reported by the participants. In particular, several participants expressed confusion on how to report the Appearance test on “Record Keeping for Pureed”. They questioned whether any “very small” lumps was acceptable. These findings support the need for multiple instruction sessions and reinforcement of learned concepts, including the expectations related to food particles, along with additional hands-on practice to develop proficiency with the processes.
| Table 1: Participants’ assessments of researcher- and participant-produced food items (N = 59.) | |||
|
Recipe |
Numbera |
Correctly completed Assessment Formsb n (%) | Items meeting Level 4 Pureed Criteriac
n (%) |
| Carrots
Assessed Immediately Assessed at 15 minutes |
19 19 |
12 (63) 11 (58) |
10 (83) 9 (82) |
| Thawed Carrots
Assessed Immediately Assessed at 15 minutes |
34 34 |
16 (47) 12 (35) |
16 (100) 12 (100) |
| Meatballs
Assessed Immediately Assessed at 15 minutes |
35 35 |
26 (74) 25 (71) |
12 (46) 11 (44) |
| Thawed Meatballs
Assessed Immediately Assessed at 15 minutes |
35 35 |
23 (66) 21 (60) |
17 (74) 13 (62) |
| Macaroni & Cheese
Assessed Immediately Assessed at 15 minutes |
19 19 |
14 (74) 11 (58) |
4 (29) 4 (36) |
| Thawed Macaroni & Cheese
Assessed Immediately Assessed at 15 minutes |
34 34 |
16 (47) 12 (35) |
10 (63) 4 (33) |
| Peaches
Assessed Immediately Assessed at 15 minutes |
35 35 |
30 (86) 33 (94) |
27 (90) 26 (79) |
| Thawed Peaches
Assessed Immediately Assessed at 15 minutes |
35 35 |
30 (86) 30 (86) |
25 (83) 25 (83) |
Note:
a Total number of student participation reflects class size and student availability as testing was completed during class time.
b Correctly completed assessment forms excluded those with missing responses or participant inability to identify whether the food item met the criteria for Level 4 pureed foods.
c Level 4 pureed foods passed or met criteria for appropriate Appearance, Fork Drip and Spoon Tilt tests. Thawed food items were researcher-produced.
Level 2 Mildly Thick Liquids
A total of 27 “Record Keeping Intended for Liquids” forms was submitted by participants, but 4 forms were not analyzed as the section for “Time of Service” samples was incorrectly completed. Of the 23 correctly completed assessments for milk at the time of service, 39% met the recommended Level 2 Mildly Thick criteria. This result may be in part due to the interpretation by participants of the manufacturer’s instructions for the thickening agent, and the variations in time lapse after milk was thickened but before tested. Of the 23 participants who correctly completed the form, 19 did so 15 minutes after the initial testing to determine if the time factor affected the viscosity/thickness of the product after using the thickening agent. It was found that after 15 minutes, 68% of the items had further thickened resulting in a product that now met the criteria for a Level 3 Moderately Thick liquid. If child nutrition departments choose to thicken beverages, time between preparation and service needs to be a consideration.
Sensory Evaluations between Recipes and Commercial Products
Results of the sensory evaluations between products made using the developed recipes and the commercial items are shown in Table 2. There were 36 students who participated in the evaluation of the spaghetti and peaches, 33 in the evaluations for the carrots, and 32 in the macaroni and cheese. Some students (≤4) chose not to evaluate every pair of food items. Participants scored the characteristics of taste, smell, appearance, and texture on a scale range of 0 (extremely dislike) to 9 (like extremely). Mean scores were calculated for each characteristic. The samples produced by the researchers (“B” Samples) consistently received higher combined mean scores for all sensory characteristics when compared to the commercial samples (“A” Samples). The higher mean taste scores for all prepared items may be in part due to a preference for the higher levels of sodium and other seasonings in the prepared samples compared to the jarred baby foods, which were used for the commercial samples.
Table 2. Mean Scores of Sensory Ratings of Commercial and Prepared Foods
Range for scores was 0-9. Some students (≤4) chose not to evaluate all paired items.
|
Food Item |
(N) |
Taste (M) | Smell (M) | Appearanc e
(M) |
Texture (M) | Total (M) | |||||
| Sample | A | B | A | B | A | B | A | B | A | B | |
|
Carrots |
33 |
4.91 |
5.94 |
4.97 |
6.09 |
4.00 |
6.39 |
5.36 |
5.88 |
4.81 |
6.07 |
| Peaches | 36 | 5.61 | 6.92 | 6.69 | 7.14 | 5.33 | 6.94 | 5.83 | 6.39 | 5.86 | 6.85 |
| Spaghetti | 36 | 3.89 | 6.50 | 4.97 | 5.69 | 4.00 | 4.46 | 4.17 | 5.31 | 4.26 | 5.49 |
| Macaroni & Cheese |
32 |
3.28 |
4.28 |
3.81 |
4.72 |
2.69 |
3.97 |
4.00 |
4.06 |
3.44 |
4.26 |
Note: A represents commercial food items; B the prepared food items
Paired Preference Test
The researcher prepared samples were the preferred choice over commercially prepared items for all paired preference evaluations. Of the 33 participants, 73% chose the prepared carrot sample, 83% (n=30) the prepared meatballs, and 75% (n=27) the prepared peach sample over the commercial counterparts. Evaluation of macaroni and cheese samples found that approximately half (56%; n=18) of the participants preferred the sample prepared from the developed recipe. It was noted that the individual sensory evaluations of these two samples yielded closer scores to each other when compared to the other food items. Overall, the results of the preference test may also be due, in part, to the higher level of seasonings in the prepared products that may have improved taste and smell as seen in the other sensory evaluation results. Furthermore, the prepared products may have been more representative of foods eaten by this age group on a regular basis.
Training and Testing Assessments
After participants completed instruction on the IDDSI guidelines and the training/testing procedures, they responded with their levels of agreement to the 15 items on the Feedback Questionnaire of Training and Testing. Results are shown in Table 3. Most participants (n=37, 63%) reported that the tests used to complete the modified IDDSI forms did not require many tools, 5% (n=3) were neutral, and 32% (n=19) were of the opinion that the procedures did require many tools. Ninety percent (n=53) of the participants thought that preparation and testing of the texture-modified recipes could be completed in a timely manner. The majority of participants agreed (92%) that the directions for making the texture-modified recipes were easy to follow and that the instructor was easy to understand (87%).
Table 3. Participants’ Level of Agreement to Statements about Recipes and Training (N=59)
| Statements | n | Agreea
n (%) |
Neutralb
n (%) |
Disagreec
n (%) |
| Procedure Items | ||||
| The preparation and testing of the texture- modified recipes requires many tools. | 59 | 19 (32) | 3 (5) | 37 (63) |
| Checking thickness quality before serving texture-modified recipes is a hassle. | 59 | 15 (25) | 2 (3) | 42 (71) |
| The preparation and testing of the texture- modified recipes was completed in a timely fashion. |
59 |
53 (90) |
3 (5) |
3 (5) |
| I had no mishaps during the development of texture-modified recipes. | 58 | 41 (70) | 2 (3) | 15 (26) |
| I had no troubles testing the consistency/texture of the texture- modified recipes. |
58 |
52 (88) |
3 (5) |
3 (5) |
| Instruction Presentation Items | ||||
| The texture-modified recipes contribute to a well-balanced diet. | 59 | 49 (83) | 8 (14) | 2 (3) |
| The new instruction will lower expenses. | 59 | 34 (58) | 23 (39) | 2 (3) |
| The directions for making texture- modified recipes is easy to follow. | 58 | 54 (92) | 0 (0) | 4 (7) |
| I felt more confused after the instruction. | 58 | 8 (14) | 6 (10) | 44 (75) |
| The instructor was easy to understand. | 57 | 51 (87) | 1 (2) | 5 (9) |
Note: aIncludes “agree” and “strongly agree” responses; b Includes “neutral” responses;
c Includes “disagree” and “strongly disagree” responses.
Limitations
While efforts were made to control the variability of food item preparation among the participants and the equipment used for this study, the researchers noted that basic kitchen skills were lacking in some participants, which may have led to preparation errors. The blenders used for pureeing were not all equivalent in power, and as a result, produced varying pureed consistency if participants did not adjust time for removal of all lumps. Also, because participants conducted the taste test after receiving the instructions on preparing the texture-modified recipes and actually preparing the recipes, they may have been able to distinguish between the prepared pureed food item and the commercial product by appearance, influencing their preference choice. Lastly, the researchers acknowledge the limitation of using proxies for child nutrition personnel.
CONCLUSIONS AND APPLICATION
To the knowledge of the researchers, this study is the first to examine the feasibility of using IDDSI guidelines and resources to guide preparation and assessment of texture-modified food items and thickened liquids outside of a healthcare setting, such as in schools. Student participants, the majority of whom had limited food laboratory skills and knowledge related to texture-modified foods, were utilized as a proxy for child nutrition food service employees. Participants with little to no training in texture-modified food preparation were able to effectively prepare and assess pureed food items and a thickened liquid following a 25 minute presentation. The majority reported positive feedback about the instructions received, procedures used to guide recipe preparation, and directions to conduct assessment of the menu items to meet IDDSI criteria. However, the success of the comparable researcher-produced samples related to meeting IDDSI criteria may be a reflection of additional practice in producing modified food items. Findings from this study support the recommendation for multiple training and practice sessions to achieve the highest rates of meeting set criteria for the desired level of texture-modification, and to improve the accuracy and documentation of testing procedures.
One advantage to being able to produce texture-modified menu items in-house is the opportunity to enhance the child nutrition departments’ provision of more acceptable food items to school children requiring these diets, with the goal of ultimately improving their nutritional intake. Food acceptance is important to achieving adequate caloric and nutrient consumption. The researchers concluded that the increased acceptability may be, in part, due to the fact that items prepared and evaluated in the study were more similar to foods commonly eaten by school age children and adolescents, and were more seasoned than the commercial product, which was jarred baby food. While there have been anecdotal reports of the use of commercial baby foods in settings where there is a very small number of students needing texture modification, it is unknown how widespread this is practiced. In a school setting, texture-modified menu items prepared by staff can also be consistent with foods offered as part of the district’s school breakfast and lunch programs, with flavors acceptable to that region of the country and the local population. Additionally, serving texture-modified foods similar to the menu items offered to all of the children may limit the feeling of isolation, as children with special dietary accommodations can consume those menu items rather than special foods. The findings in this study support a preference for in-house produced menu items rather than commercially prepared foods. Additional testing by school districts with their students could provide more accurate insights into children’s preferences.
While not a focus of this study, in-house, prepared texture-modified food items could offer a lower-cost alternative to commercially prepared products and may assist child nutrition departments with meeting budget guidelines. Batch production and freezing of food items may be preferable to schools with fewer students needing texture modification while production in a central facility and distribution to schools may be desirable to school districts who choose to share these items within a district. It may also be possible to batch-freeze items that are re-occurring on a cycle menu. The freezing, thawing, and assessment of the researcher prepared items allowed participants to simulate the scenario where this process would be implemented. Batch-freezing may also save employee labor, time, and cost.
An unexpected finding of this study related to the use of the commercial thickener was the increase in thickness of the milk after sitting for 15 minutes. Testing by the child nutrition programs with their chosen commercial thickener is recommended, as thickeners may vary between manufacturers. Results may impact the timing of the liquid preparation and meal service for the student meal, and knowledge would allow for efficient production. Currently, instructions on the label of the thickening agent include a range in the time following its addition to liquids and the time of service. It may take time for manufacturers to include label updates to reflect the IDDSI categories for levels of thickness that will be consistent with diet modification orders. For the beverage component of the meal or snack, child nutrition programs may choose to prepare the beverage on site regardless of where the food items are being prepared, and they may also be able to purchase commercial pre-thickened liquids, if not cost- prohibitive.
This effort to assess the feasibility of using the IDDSI resources as a foundation for developing training materials and procedures in non-healthcare settings, such as child nutrition programs in schools, was a preliminary effort. Future research should be conducted with child nutrition program personnel most likely to prepare texture-modified items in accordance with the use of the IDDSI instructional materials and criteria testing procedures in a variety of food service production systems. The variation in IDDSI levels for the food and liquid items reported in this study emphasizes the importance of standardizing texture and consistency levels. Findings from this study also support the need for training and practice with IDDSI resources for child nutrition personnel responsible for meal accommodations to ensure compliance with diet prescriptions and the safety of the child receiving the school meal or snack.
Overall, findings of this preliminary work build support for incorporating IDDSI guidelines for producing and assessing texture-modified foods and beverages in school-based child nutrition operations. These processes could increase the safe delivery of food and beverages to students with dysphagia, potentially increase food acceptance, and ultimately, improve the nutritional status of the students.
References
American Speech Language Hearing Association. (2017). Pediatric Dysphagia. Retrieved from
https://www.asha.org/PRPSpecificTopic.aspx?folderid=8589934965§ion=Incidence
_and_Prevalence
Amunrud, E. A., Mitchell, C. O., & Sun, M. M. (1999). Acceptability and Health Effects of
Commercially Prepared Puree Foods in Nursing Home Residents. Journal of the
American Dietetic Association, 99(9, Supplement), A119. https://doi.org/10.1016/S0002-
8223(99)00813-5
Arvedson, J. C. (2008). Assessment of pediatric dysphagia and feeding disorders: clinical and
instrumental approaches. Developmental Disabilities Research Reviews, 14(2), 118–127.
https://doi.org/10.1002/ddrr.17
DeSantos, F. A., Ramamoorthi, L., Bechtel, P., Smiley, S., & Brewer, M. S. (2010). Effect of
Salmon Type and Presence/Absence of Bone on Color, Sensory Characteristics, and
Consumer Acceptability of Pureed and Chunked Infant Food Products. Journal of Food
Science, 75(6), S279–S285. https://doi.org/10.1111/j.1750-3841.2010.01709.x
Dodrill, P. & Gosa, M. M. (2015) Pediatric Dysphagia: Physiology, Assessment, and
Management. Annals of Nutrition and Metabolism; 66(Supplement 5):24-3.
https://doi.org/10.1159/000381372
Edgar, D. L., & Rosa-Lugo, L. I. (2007). The critical shortage of speech-language pathologists in
the public school setting: features of the work environment that affect recruitment and
retention. Language, Speech, and Hearing Services In Schools, 38(1), 31–46.
Failure to Thrive. (n.d.). Retrieved October 8, 2017, from
http://www.stanfordchildrens.org/en/topic/default?id=failure-to-thrive-90-P02297
Germain, I., Dufresne, T., & Gray-Donald, K. (2006). A Novel Dysphagia Diet Improves the
Nutrient Intake of Institutionalized Elders. Journal of the American Dietetic Association,
106(10), 1614–1623. https://doi.org/10.1016/j.jada.2006.07.008
Guerrero, K., Olsen, A., & Wistoft, K. (2018). What Role Does Taste Play in School Meal
Studies? A Narrative Review of the Literature. Journal of Child Nutrition &
Management, 42(1): 1-16.
Hayes, D., Contento, I. R., & Weekly, C. (2018). Position of the Academy of Nutrition and
Dietetics, Society for Nutrition Education and Behavior, and School Nutrition
Association: Comprehensive Nutrition Programs and Services in Schools. Journal of The
Academy Of Nutrition And Dietetics, 118(5), 913–919. https://doiorg.ezproxy.shsu.edu/10.1016/j.jand.2018.03.005
Hoffman, V., Srinivasan, M., Levin, M. & Scarmo, S. (2018). Operating School Meal Programs
in Rural Districts: Challenges and Solutions. Journal of Child Nutrition & Management,
42(1): 1-11.
Holben, D. H. (2010). Position of the American Dietetic Association: Food insecurity in the
United States. Journal of The American Dietetic Association, 110(9), 1368–1377.
Homer, E. M. (2008). Establishing a public school dysphagia program: A model for
administration and service provision. Language, Speech, and Hearing Services In
Schools, 39(2), 177–191. https://doi.org/10.1044/0161-1461(2008/018)
Homer, E., & Carbajal, P. (2015). Swallowing and feeding services in the schools: from therapy
to the sinner table. Perspectives on Swallowing and Swallowing Disorders (Dysphagia).
24: 155-161. Retrieved on May 4, 2018 from pediatricfeedingnews.com/wpcontent/uploads/2016/03/Homer-article-pdf
IDDSI (2016). IDDSI, International Dysphagia Diet Standardisation Initiative. Retrieved
September 25, 2018 from: http://iddsi.org/
Lepore, J. R., Sims, C. A., Gal, N. J., & Dahl, W. J. (2014). Acceptability and Identification of
Scooped Versus Molded Puréed Foods. Canadian Journal of Dietetic Practice and Research: A Publication of Dietitians of Canada = Revue Canadienne De La Pratique Et
De La Recherche En Dietetique: Une Publication Des Dietetistes Du Canada, 75(3), 145–
147. https://doi.org/10.3148/cjdpr-2014-004
Matsuo, K. & Palmer, J.B. (2008). Anatomy and physiology of feeding and swallowing – normal
and abnormal. Physical Medicine and Rehabilitation Clinics of North America, 19(4),
691–707. doi:10.1016/j.pmr.2008.06.001.
McLaughlin, G. (1969). SMOG grading: A new readability formula. Journal of Reading, 12 (8),
639-64.
National Institute on Deafness and other Communication Disorders, National Institutes of Health
(2010). Dysphagia (NIH Pub. No. 13-4307). Retrieved from
https://www.nidcd.nih.gov/health/dysphagia
United States Department of Agriculture Food and Nutrition Service [USDA]. (2017)
Accommodating children with disabilities in the school meal programs: guidance for
school food service professionals (USDA Doc No. SP40-2017). Retrieved from
https://fns-prod.azureedge.net/sites/default/files/cn/SP40-2017a1.pdf
Vaclavik, V. A., & Christian, E. W. (2014). Essentials of Food Science. New York, NY:
Springer New York.
Wadhera, D., & Capaldi-Phillips, E. D. (2014). A review of visual cues associated with food on
food acceptance and consumption. Eating Behaviors, 15(1), 132–143.
https://doi.org/10.1016/j.eatbeh.2013.11.003
Werthmann, J., Jansen, A., Havermans, R., Nederkoorn, C., Kremers, S., & Roefs, A. (2015).
Bits and pieces. Food texture influences food acceptance in young children. Appetite,
84(Supplement C), 181–187. https://doi.org/10.1016/j.appet.2014.09.025
Biography
Catherine Shaw, MS, RDN, and McKenzie Moore, MS, MBA, RDN, are former Graduate Students at Sam Houston State University. Corresponding Author Simone Camel, PhD, RDN, is Assistant Professor, Food & Nutrition and the Adelaide Murdock Hunt Endowed Professor in the School of Human Ecology at Louisiana Tech University, Ruston, Louisiana. Corresponding Author Crystal Clark Douglas, PhD, RDN, is Associate Professor in the Department of Nutrition & Metabolism at The University of Texas Medical Branch in Galveston, Texas.
Purpose / Objectives
Children with developmental disorders may require texture-modified diets. The purpose of this study was to determine if materials developed by the International Dysphagia Diet Standardization Initiative (IDDSI) are feasible for use by child nutrition personnel.